manhattan life dental claim form
Health Policy Cancellation Form. 247 patient benefit verification claims and remittance statements.
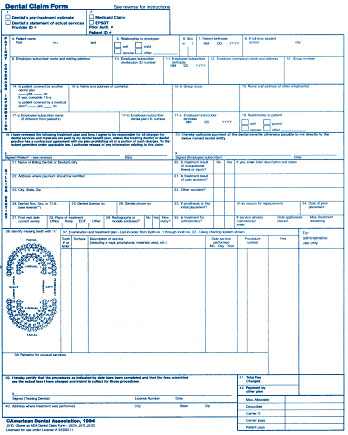
Insurance Claim Forms Dental Continuous Feed Dental Insurance Claim Forms Dental Forms Medical Forms
For additional information about dental vision and hearing insurance or any.

. DENTISTS STATEMENT OF ACTUAL. For Assistance please call1-888-441-07708am - 5pm CST. Or contact our Customer Service department.
Signature If Claim Is For A Minor Parent Or Legal Guardian Must Sign Date Submit Completed Form to. Signature If Claim Is For A Minor Parent Or Legal Guardian Must Sign Date Submit Completed Form to. For Assistance please call1-888-441-07708am - 5pm CST.
To process a claim please. APercentage of Basic eye exam or eye refraction. Submit Completed Form to.
Central United Life Insurance Company was formed in 1963 a subsidiary of Central Mutual Insurance. Select the appropriate form category below. Box 925309 Houston TX 77292-5309 Customer Service.
Select the appropriate form category to the right. Visit the ContractPolicy Holder. Bank Draft Authorization Form In English.
Health Screening Benefit Claim Form ManhattanLife Claims PO. Need to file a Voluntary Benefits Group Policy Claim. Dental Vision and Hearing Insurance C-DVH 0615 A plan with choices for you and your family Not available in all.
Manhattan life dental claim form Wednesday February 9 2022 Edit. 1-800-669-9030 Annuity Contract Owners. Signature Printed Name.
VB Accident Claim Form. Box 925309 Houston TX 77292-5309 Customer Service. HIPAA Form release PHI.
The Easy Upload mobile app or the Easy Form Upload tool found on the Client. Manhattan life dental claim form Monday August 8 2022 Edit. VB Life Claim Form.
In 1993 they were acquired by. Affidavit of Lost Policy - International Life Policies. ManhattanLife VB Claims Department PO Box 926169 Houston TX 77292.
Bank Draft Authorization Form In English en Español Beneficiary Change Form. Life Health Policyholders. Report a Death Claim Online Form Acknowledgement of Misplaced Policy.
ManhattanLife VB Claims PO Box 926169 Houston TX 77292 Customer Care. Affidavit of Lost Policy Form. ManhattanLife VB Claims PO Box 926169 Houston TX 77292 Customer Care.
Benefit exclusions and limitations may apply to the policy. EASY UPLOAD MOBILE APP. Annuity Cash Value and Maturity Value Request.
What is ManhattanLife Central United Life. Dental Vision and Hearing Insurance. Duplicate Policy Request Form.

Manhattanlife Manhattanlifeco Twitter
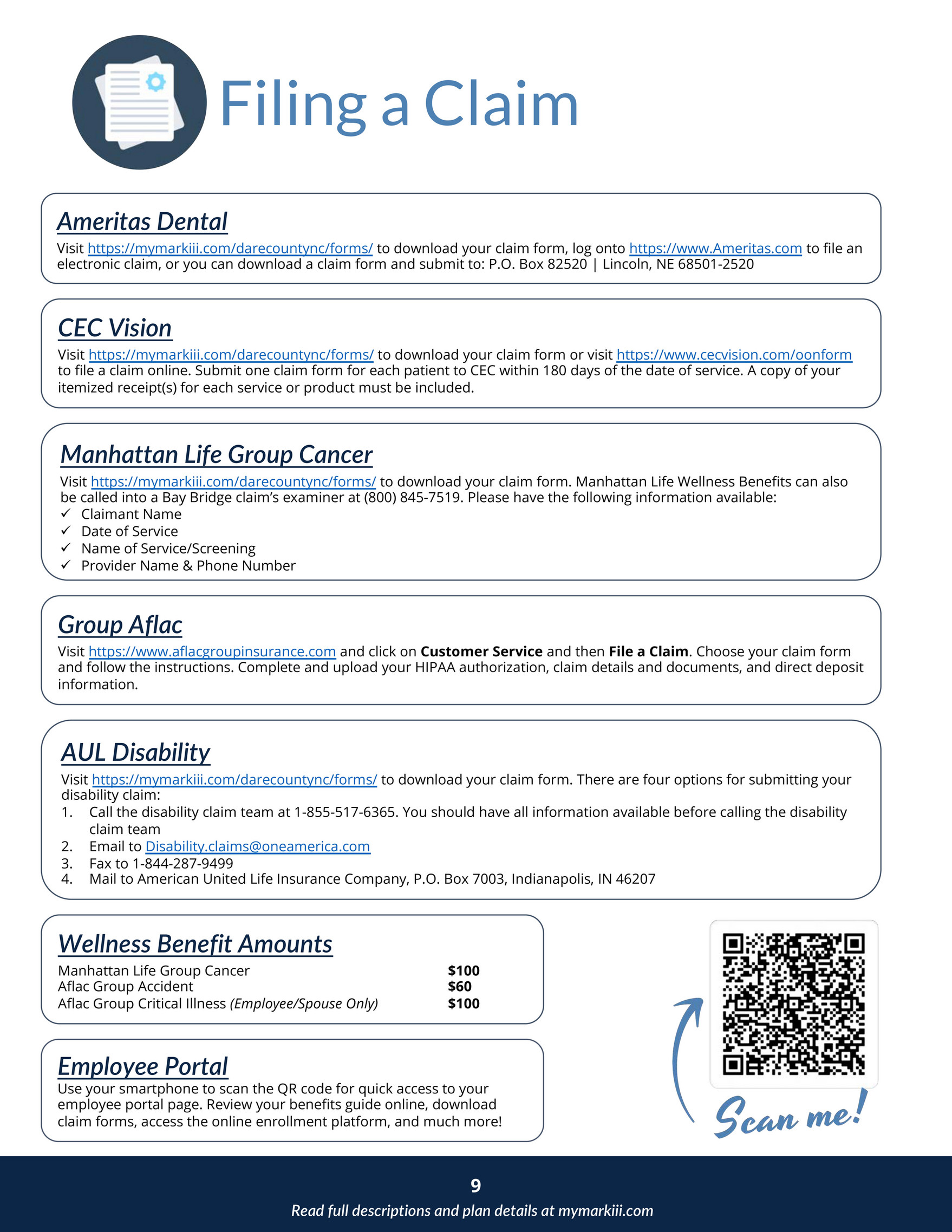
Mark Iii Employee Benefits Dare County Benefits Booklet Page 4 5 Created With Publitas Com
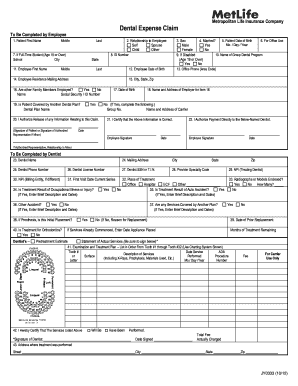
2018 2022 Form Metlife Jy0333 Fill Online Printable Fillable Blank Pdffiller

Manhattanlife Client Services
![]()
Dental Vision And Hearing Insurance Dvh Manhattanlife

Manhattanlife Manhattanlifeco Twitter
![]()
Dental And Vision Insurance Plans For Nomads Nomad Insurance Group

3idjdpfwkreo7m

Standard Ada Form Fill Online Printable Fillable Blank Pdffiller
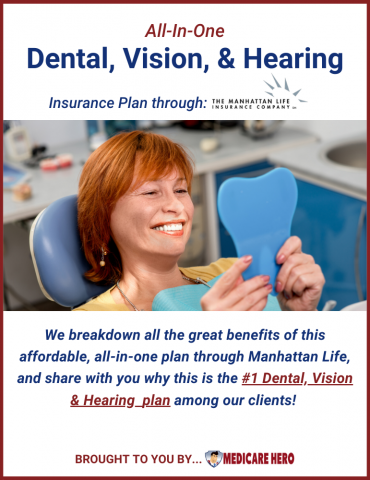
Dental Insurance Medicare Hero

Manhattan Life Insurance Company Dental Vision Hearing Review Youtube

Manhattanlife Reviews 425 Reviews Of Manhattanlife Com Sitejabber
![]()
Dental Vision And Hearing For Seniors Manhattanlife
Do You Have New Dental Insurance Coverage Santa Monica Ca

Manhattanlife Manhattanlifeco Twitter

Family Life Insurance Company Review
Manhattanlife Reviews 425 Reviews Of Manhattanlife Com Sitejabber

Manhattan

Dental Vision And Hearing Insurance Senior Benefits Of Georgia